
One of the most common medical diagnoses today is high blood pressure or hypertension, but what does the term actually mean and what are the real risks associated with hypertension. It is true that elevated blood pressure does increase your risk of cardiovascular disease (CVD)* however the actual numbers may surprise you. The issue arises as we use terms like high, moderate and low risk in the mainstream and in medicine without specifically defining them or putting them into context. Once these risks are defined the benefits of the treatments can be described to the patient in terms of risk reduction as opposed to focusing on a decreasing the blood pressure which is a surrogate marker and has no actual meaning other than quantifying risk.
Risk assessment can be done using several tools, the most popular being the Framingham Scale (2) which takes in to account cholesterol levels and calculates a 10 year risk of developing coronary heart disease (CHD)** and more recently a 5 year risk calculator for CVD from the Lancet (3) that is done without the use of cholesterol levels. It is useful to put numbers to the different classifications of risk as each person’s definition of high, moderate or low will vary greatly. Those in the ‘High Risk’ category as defined by Lancet have a 30% or greater chance of developing CVD over a 5 year period. The ‘Moderate Risk’ group using the same scale ranges from a 10-30% chance of CVD over 5 years and the ‘Low Risk’ group has a 5-10% chance of developing CVD in 5 years. The Framingham scale uses similar categories for CHD over a 10 year period creating a baseline risk using your age and modifying that risk depending on several factors listed below. According to this scale, at age 50 your risk starts at 4%, at age 60 your risk is 6% and at 70 years old your risk begins at 10% over the next 10 years. These numbers are a baseline and factors such as gender, high cholesterol levels, smoking, elevated blood pressure, family history of CVD and diabetes will increase your risk accordingly.
Risk assessment can be done using several tools, the most popular being the Framingham Scale (2) which takes in to account cholesterol levels and calculates a 10 year risk of developing coronary heart disease (CHD)** and more recently a 5 year risk calculator for CVD from the Lancet (3) that is done without the use of cholesterol levels. It is useful to put numbers to the different classifications of risk as each person’s definition of high, moderate or low will vary greatly. Those in the ‘High Risk’ category as defined by Lancet have a 30% or greater chance of developing CVD over a 5 year period. The ‘Moderate Risk’ group using the same scale ranges from a 10-30% chance of CVD over 5 years and the ‘Low Risk’ group has a 5-10% chance of developing CVD in 5 years. The Framingham scale uses similar categories for CHD over a 10 year period creating a baseline risk using your age and modifying that risk depending on several factors listed below. According to this scale, at age 50 your risk starts at 4%, at age 60 your risk is 6% and at 70 years old your risk begins at 10% over the next 10 years. These numbers are a baseline and factors such as gender, high cholesterol levels, smoking, elevated blood pressure, family history of CVD and diabetes will increase your risk accordingly.

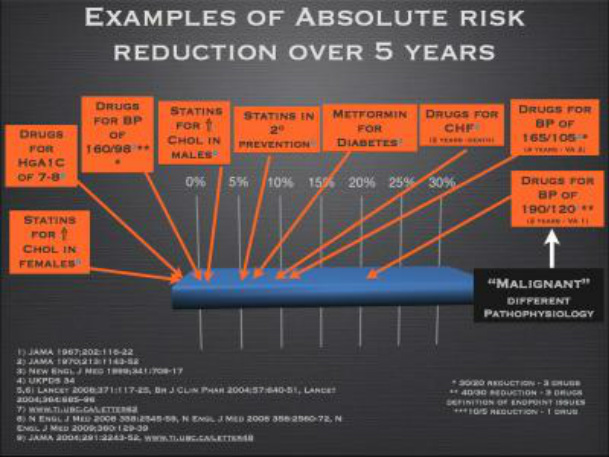
Now that we have defined the chances of developing CVD or CHD over a 5 and 10 year period, we will take a look at the effects of blood pressure lowering medications and their exact numbers in relation to decreasing the risk of all-cause mortality***. All of the following numbers are in relation to primary prevention which means that the patient has not been diagnosed with CVD or had a previous myocardial infarction also known as a heart attack. As an example to put this in to context we will look at the absolute reduction (AR) of the risk for someone who has a blood pressure starting at 160/90 mmHg before treatment and reduced to 145/85 mmHg using only one drug. The absolute risk reduction this person will receive over a 5 year period will be 1-3%. This means that if the risk started at 20% with no treatment it would be decreased to 17% after 5 years of drug therapy (Appendix A). All classes of blood pressure lowering medications have been shown to have similar absolute risk reductions of all-cause mortality (4). However, the higher your risk is to begin with the greater benefit you will see from the medication and I encourage everyone to calculate your own approximate risk of CVD and the absolute benefit you will receive from therapy.
Elevated blood pressure is becoming more common as the guidelines are changed and standards lowered and it can be reduced through many interventions including diet and lifestyle changes. One example of past standards is a study published by the Lancet in 1966 which contained patients with an average blood pressure of 200/110 mmHg and the title of that study is “The Effects of Propranolol on MILD hypertension.” If that blood pressure were measured in a patient today they would be sent immediately to the emergency room. It may take time to lower your blood pressure and your readings will vary from day to day so it is best not to measure each day as this may cause stress and elevated readings for some. Two or three readings per month are enough to get an average measurement and a better overview of where your blood pressure truly stands. This article is not meant to defer people from taking their medication. We only wish to inform patients of the actual benefits of their medications. Some may find the risk reduction to be of great value and others may believe that it is not worth the trouble of taking a medication each day (which may come with some unwanted side effects). We support both opinions and encourage patients to make the final decision on their own using all of the information available. Before starting, stopping or altering any of your medications please speak to your health care professional.
*Cardiovascular disease refers to any disease of the blood vessels or heart and includes stroke, heart attack, peripheral vascular disease and coronary heart disease.
**Coronary heart disease refers to blockage of arteries that supply blood to the heart.
***All-cause mortality is defined as death from any cause.
References
1. McCormack, J. and Allan, M. (2008) Therapeutics Education Collaboration Podcast. Episodes 3-12.
2. http://www.framinghamheartstudy.org/risk/coronary.html
3. Gaziano, T., Young, C., Fitzmaurice, G., Atwood, S. and Gaziano, J.M. (2008) Laboratory-based versus non-laboratory-based method for assessment of cardiovascular disease risk. The Lancet; 371:923 – 31.
4. The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. (2002). Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs. Diuretic. JAMA; 288(23):2981- 97.
Elevated blood pressure is becoming more common as the guidelines are changed and standards lowered and it can be reduced through many interventions including diet and lifestyle changes. One example of past standards is a study published by the Lancet in 1966 which contained patients with an average blood pressure of 200/110 mmHg and the title of that study is “The Effects of Propranolol on MILD hypertension.” If that blood pressure were measured in a patient today they would be sent immediately to the emergency room. It may take time to lower your blood pressure and your readings will vary from day to day so it is best not to measure each day as this may cause stress and elevated readings for some. Two or three readings per month are enough to get an average measurement and a better overview of where your blood pressure truly stands. This article is not meant to defer people from taking their medication. We only wish to inform patients of the actual benefits of their medications. Some may find the risk reduction to be of great value and others may believe that it is not worth the trouble of taking a medication each day (which may come with some unwanted side effects). We support both opinions and encourage patients to make the final decision on their own using all of the information available. Before starting, stopping or altering any of your medications please speak to your health care professional.
*Cardiovascular disease refers to any disease of the blood vessels or heart and includes stroke, heart attack, peripheral vascular disease and coronary heart disease.
**Coronary heart disease refers to blockage of arteries that supply blood to the heart.
***All-cause mortality is defined as death from any cause.
References
1. McCormack, J. and Allan, M. (2008) Therapeutics Education Collaboration Podcast. Episodes 3-12.
2. http://www.framinghamheartstudy.org/risk/coronary.html
3. Gaziano, T., Young, C., Fitzmaurice, G., Atwood, S. and Gaziano, J.M. (2008) Laboratory-based versus non-laboratory-based method for assessment of cardiovascular disease risk. The Lancet; 371:923 – 31.
4. The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. (2002). Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs. Diuretic. JAMA; 288(23):2981- 97.
Appendix A
 RSS Feed
RSS Feed